12-Facility LTC Network Achieves 99.4% MDS First-Pass Accuracy

Two facilities in Heritage Care’s 24-facility network were flagged for CMS targeted surveys in the same quarter. Leadership gave the CMO a 90-day window to prevent further escalation.
Business Challenges
The call to the CMO came on a Friday afternoon. The administrator at the Bismarck facility reported a CMS notice for a targeted survey tied to MDS accuracy concerns raised in quarterly quality measures. It was the second such notification in six weeks, following a similar case at the Sioux Falls facility.
The network president escalated the issue over the weekend, warning that a third targeted survey could trigger a broader regional CMS review. That would likely slow admissions across the network and create financial and regulatory risk. He requested a clear understanding of the issue and whether it could be resolved within 90 days.
The CMO identified the root issue as variability in MDS execution across facilities. Heritage Care had grown through acquisitions over five years, but RAI processes had not been standardized. First-pass MDS accuracy averaged 78% across the network, with some facilities as low as 64%. PDPM reimbursement was not fully aligned with case mix due to under-documentation in Nursing and NTA components. Survey findings also cited mismatches between care plans and documentation.
- Two targeted CMS surveys in six weeks due to MDS accuracy concerns; risk of additional regulatory escalation.
- Network-wide MDS first-pass accuracy averaged 78%, with low-performing facilities at 64%.
- PDPM revenue lagged case-mix complexity by ~11% due to under-coding in key components.
- Care plan documentation inconsistencies were flagged in audits across multiple facilities.
- MDS quality visibility was limited, with reporting available only on a monthly basis.
Solution
The CMO led a fast-track procurement focused on operational speed and real-time visibility. The priority was a platform that could deliver measurable MDS improvements within 90 days and provide facility-level visibility within the first month.
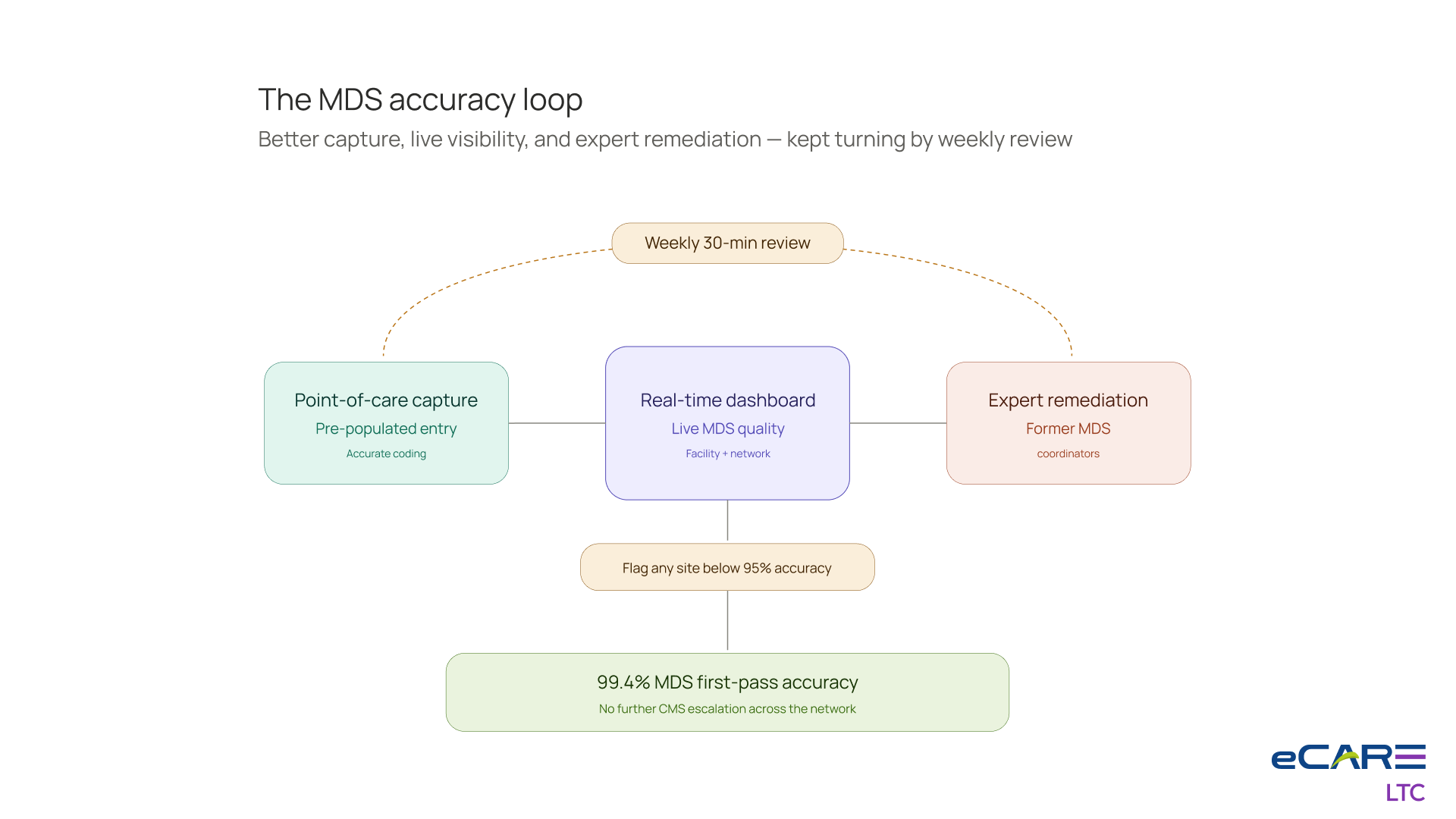
eCareLTC was selected based on its ability to enable live MDS quality tracking and point-of-care documentation support. The platform’s pre-population capabilities were deployed to reduce manual entry and improve coding accuracy during assessment workflows. A real-time dashboard provided visibility into MDS performance at both facility and network levels within 30 days.
A key factor in the decision was the availability of clinical-services expertise within the vendor team, including former MDS coordinators. This allowed close operational alignment with internal teams during rollout and ensured workflow-level adoption rather than system-only implementation.
Value Delivered
Within 90 days, the network achieved its performance targets and avoided additional CMS escalation. MDS quality and documentation consistency improved across all facilities.
- MDS first-pass accuracy improved from 78% to 99.2% across the network; lowest-performing facility reached 96%.
- PDPM revenue increased by 11% through improved documentation alignment with case mix.
- No additional CMS targeted surveys occurred in the 12 months following deployment.
- MDS coordinator workload decreased from 14 hours to 6 hours per assessment.
- Real-time MDS quality dashboards became standard in all facility leadership meetings.
Solution Provided
The deployment was executed in phases, starting with high-risk facilities and expanding across the network based on performance tiers.
Days 1–7: Crisis Triage at Sioux Falls and Bismarck
The first phase focused on the two flagged facilities. Existing MDS data was analyzed to identify error patterns and high-risk assessment areas. This established a baseline for targeted correction efforts.
Weeks 2–4: Configuration + MDS Coordinator Workflow at the Two Facilities
MDS coordinators worked with eCareLTC clinical teams to align workflows with facility-specific case mix requirements. Real-time dashboards were activated within two weeks, enabling immediate visibility into documentation quality.
Weeks 5–8: Facilities 3–8 (The Highest-Risk Tier)
Six additional high-risk facilities were onboarded in pairs. Training focused on improving consistency in assessment workflows and standardizing documentation practices.
Weeks 9–13: Facilities 9–18 (The Mid-Tier)
Ten mid-tier facilities were deployed in phases. By this stage, implementation patterns were standardized, enabling faster onboarding and stabilization across sites.
Weeks 13–16: Facilities 19–24 (The Best-Performing Tier)
The remaining higher-performing facilities were activated. These sites required workflow alignment rather than remediation, with a focus on maintaining consistency across the network.
The Network Dashboard Discipline
A weekly 30-minute MDS performance review was introduced starting week 4. Facility leaders were required to review accuracy metrics and submit remediation plans for any site falling below 95% accuracy. This created consistent accountability across the network.
Business Value
The CMO presented full-year results to the board in late 2025, focusing on both regulatory stability and financial impact.
What changed about CMS risk posture
Following the improvements, the network moved from elevated monitoring to standard CMS oversight within two quarters. This reduced regulatory risk and protected planned expansion activity, including pending acquisitions.
The financial picture
Improved documentation quality contributed approximately $14M in annual incremental PDPM revenue. Additional efficiency gains reduced administrative burden across facilities. Total implementation cost was approximately $1.2M.
What changed about MDS as a discipline
MDS management shifted from a back-office compliance function to a core operational discipline tied directly to revenue and regulatory performance. The role of MDS coordinator was elevated, and a new Network MDS Director position was created reporting to the CMO.
The PDPM revenue line
The revenue uplift reflects improved alignment between documentation and clinical complexity. While financially significant, leadership emphasized that the primary outcome was reduced regulatory exposure and improved survey readiness.
What the network president said at the board meeting
“Twelve months ago, we were at risk of a regional CMS review. The organization responded within 90 days and stabilized performance. The focus now is maintaining consistency across the network and avoiding regression.”

